Symptoms and Treatment of Endometriosis.
Endometriosis -- The Silent Invader
Endometrial tissue, whether it is inside or outside the uterus, responds to the rise and fall of estrogen and progesterone produced by the ovaries during the reproductive cycle. Under the influence of the hormones, the misplaced tissue swells; and when hormonal levels drop, the tissue may bleed. Unlike the normally situated endometrium, which is shed from the body as menstrual discharge, this blood and tissue has no outlet. It remains to irritate the surrounding tissue.endometriosis ( "endo") is a common disorder that affects women of reproductive age. It occurs when normal endometrial tissue (the lining of the uterus) grows outside the uterus. This misplaced tissue may implant itself and grow anywhere within the abdominal cavity.
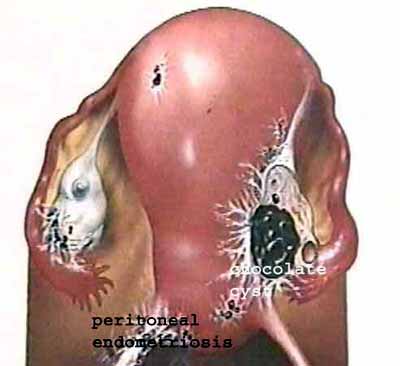
Fig 1. Schematic, showing a chocolate cyst (endometrioma) in the right ovary; and peritubal adhesions because of endometriosis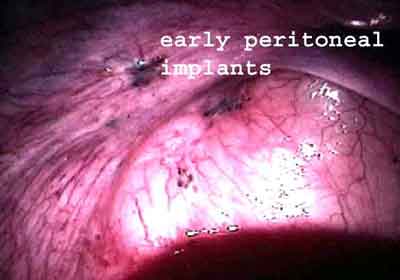
Fig 2. Laparoscopy, showing minimal endometriosis, in the form of " powder-burn" deposits.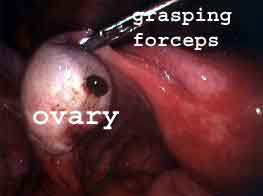
Fig 3 . Laparoscopy, showing a small chocolate cyst in the left ovary. This can be very easy to miss, so a careful multiple puncture laparoscopy is essential to make an accurate diagnosis of endometriosis.
Endometriosis can often be suspected on the basis of your symptoms. Your doctor may make a tentative diagnosis if you complain of progressively severe menstrual cramps or pain with intercourse. For many patients , making the diagnosis is a big relief – the pain I feel is not all in my head - I have a disease which is causing me to be miserable ! However, this diagnosis can come like a blow as well - especially when you read on the net about all the possible complications which endometriosis can cause ! The good news is that endometriosis does not lead to cancer; and we have may very effective treatment options to manage this.
Some patients with the condition have no discomfort at all. This is why in the past, a laparoscopy was the gold standard for making the diagnosis of endometriosis, as this allowed the doctor to actually inspect the pelvic contents and "stage" the severity of the disease. The mainstay of treatment also used to be laparoscopy. However, because it involves surgery, many infertility specialists no longer advise laparoscopy for their patients.
Ultrasound scanning is an excellent way of diagnosing chocolate cysts and can pick up cysts which are very small. On scanning, chocolate cysts are complex masses ( which have both solid and cystic components); and are often tender. They can vary in size from a few mm to over 10 cm; and can be bilateral. However, it’s not possible to make a definitive diagnosis of endometriosis on ultrasound scanning, as many other conditions can also produce cysts in the ovary. The diagnosis can be confirmed either by aspirating the cyst under ultrasound guidance ( and finding the typical dark old blood which is diagnostic of endometriosis); or by doing a laparoscopy.
Treating endometriosis with medicines has definite limitations. Medication usually controls mild or moderate pain and may eliminate small patches of the disease. But large chocolate cysts in the ovary are less likely to respond, and drugs cannot remove scar tissue. This is why surgery may be needed to improve fertility by removing adhesions, lesions, nodules or endometriomas.
This is still a vexed and controversial issue. While many gynecologists feel that operative laparoscopy should be the first choice, in reality there is little evidence to support this stance. While laparoscopy is useful for "treating" the endo lesions, whether this actually helps to improve fertility is still unproven ! In fact, overenthusiastic surgery can often push an infertile patient from the frying pan into the fire ! Unnecessary surgery reduces your fertility as normal ovarian tissue is also removed along with the cyst wall, thus reducing your ovarian reserve.
I suggest that patients always test their AMH level ( a simple blood test for checking their ovarian reserve ) before allowing a doctor to do an operative laparoscopy to treat their endometriosis. This is especially true for: older women; women who have had surgery earlier; women with recurrent cysts; and women with large ovarian cysts ( because they are at risk for having poor ovarian reserve, a silent condition called oopause.) If they do have poor ovarian reserve ( as suggested by a high FSH level and a low AMH level), then surgery is not a good idea and they should move onto IVF directly.
If there is a cyst, this can always be treated by aspirating it under vaginal ultrasound guidance, so that the ovarian reserve is not further impaired.
Endometriosis -- The Silent Invader
Endometriosis ( "endo") is a common disorder that affects women of reproductive age. It occurs when normal endometrial tissue (the lining of the uterus) grows outside the uterus. This misplaced tissue may implant itself and grow anywhere within the abdominal cavity.
Many specialists feel that severe endometriosis is more likely to be found in infertile women who have delayed pregnancy and for this reason, the condition is sometimes labeled a "career woman's disease".
Many specialists feel that severe endometriosis is more likely to be found in infertile women who have delayed pregnancy and for this reason, the condition is sometimes labeled a "career woman's disease".
Endometrial tissue, whether it is inside or outside the uterus, responds to the rise and fall of estrogen and progesterone produced by the ovaries during the reproductive cycle. Under the influence of the hormones, the misplaced tissue swells; and when hormonal levels drop, the tissue may bleed. Unlike the normally situated endometrium, which is shed from the body as menstrual discharge, this blood and tissue has no outlet. It remains to irritate the surrounding tissue.
The disease is highly unpredictable. Some women may have just a few isolated implants that never spread or grow, while in others the disease may spread throughout the pelvis. Endometriosis irritates surrounding tissue and may produce web like growths of scar tissue called adhesions. The scar tissue can bind the pelvic organs and even cover them entirely. Many women who have endometriosis experience few or no symptoms. However, in some women, endometriosis may cause severe menstrual cramps, pain during intercourse, and infertility.
It is a disease which has been called an "enigma wrapped inside a mystery ", and there is a lot about it that we do not understand as yet.
Several theories exist as to how endometriosis begins. One possibility is retrograde menstruation, the backward flow of the menstrual discharge through the fallopian tubes into the pelvis. According to this theory, the endometrial cells may implant on the ovaries or elsewhere in the pelvic cavity.
What does endometriosis look like ?
Early implants look like small, flat dark patches or flecks of blue or black paint ( "powder-burns" ) sprinkled on the pelvic surfaces. The small patches may remain unchanged, become scar tissue or spontaneously disappear over a period of months. Endometriosis may invade the ovary, producing blood filled cysts called endometriomas. With time, the blood darkens to a deep, reddish brown or tarry color, giving rise to the description "chocolate cyst." These may be smaller than a pea or larger than a grapefruit.
In some cases, bands of fibrous tissue called adhesions may bind the uterus, tubes, ovaries, and nearby intestines together. The endometrial tissue may also grow into the walls of the intestine - but although it may invade neighboring tissue, endometriosis is not a cancer.
Fig 1. Schematic, showing a chocolate cyst (endometrioma) in the right ovary; and peritubal adhesions because of endometriosis
Fig 2. Laparoscopy, showing minimal endometriosis, in the form of " powder-burn" deposits.
Fig 3 . Laparoscopy, showing a small chocolate cyst in the left ovary. This can be very easy to miss, so a careful multiple puncture laparoscopy is essential to make an accurate diagnosis of endometriosis.
What are the symptoms of endometriosis ?
What are the symptoms?
Progressively increasing dysmenorrhea (periods pains or menstrual cramping) may be a symptom of endometriosis. These are caused by contractions of uterine muscle initiated by prostaglandins released from the endometrial tissue. A puzzling feature of endometriosis is that the degree of pain it causes is not related to the extent of the disease. Some women with extensive disease feel no pain at all. A woman with endometriosis may notice that as the disease progresses her periods become more painful or that the pain begins earlier or lasts longer.
Progressively increasing dysmenorrhea (periods pains or menstrual cramping) may be a symptom of endometriosis. These are caused by contractions of uterine muscle initiated by prostaglandins released from the endometrial tissue. A puzzling feature of endometriosis is that the degree of pain it causes is not related to the extent of the disease. Some women with extensive disease feel no pain at all. A woman with endometriosis may notice that as the disease progresses her periods become more painful or that the pain begins earlier or lasts longer.
Endometriosis can cause pain during intercourse, a condition known as dyspareunia. The thrusting motion of the penis can produce pain in an ovary bound by scar tissue to the top of the vagina or in a tender nodule of endometriosis. Most women who have endometriosis report no bleeding irregularities. Occasionally, however, the disease is accompanied by vaginal bleeding at irregular intervals; or by premenstrual spotting.
How does endometriosis cause infertility ?
How does endometriosis cause infertility? The relationship between mild (early) endometriosis and infertility is controversial. The most recent theories regarding the endometriosis-infertility link focus on the fact that endometriosis may lead to a form of mild inflammation within the pelvis. In some women with mild endometriosis, the levels of certain chemicals called cytokines ( released in response to inflammation) are increased in the abdominal cavity, and these hormones may have a negative effect on follicle and egg development, egg-sperm binding and fertilization, normal tubal function, and even implantation. Sometimes, the endometriosis may be coincidental and unrelated to the fertility problem. In these patients, other factors may be involved in a couple's infertility, such as poor quality sperm or ovulation disorders- and the endometriosis is a "red herring". Some women who have the condition are able to conceive, while others may be infertile due to endometriosis or a combination of factors.
The disease may hinder conception in various ways - especially when it is severe. Endometriosis may inflame surrounding tissue and spur the growth of scar tissue or adhesions. Bands of scar tissue may bind the ovaries, fallopian tubes, and intestines together and thus interfere with the release of eggs from the ovaries or the ability of the tube to pick up the egg. Rarely, severe endomteriosis may cause the tubes to become blocked. The presence of chocolate cysts in the ovary may also impair ovulation.
How does the doctor diagnosis endometriosis ?
Ultrasound scanning is an excellent way of diagnosing chocolate cysts and can pick up cysts which are very small. On scanning, chocolate cysts are complex masses ( which have both solid and cystic components); and are often tender. They can vary in size from a few mm to over 10 cm; and can be bilateral. However, it’s not possible to make a definitive diagnosis of endometriosis on ultrasound scanning, as many other conditions can also produce cysts in the ovary. The diagnosis can be confirmed either by aspirating the cyst under ultrasound guidance ( and finding the typical dark old blood which is diagnostic of endometriosis); or by doing a laparoscopy.
What medications are used for treating endometriosis ?
Hormone medication
The goal of hormonal treatment is to simulate pregnancy or menopause, two natural conditions known to inhibit the disease. In each case, the normal endometrium is no longer stimulated to grow and regress with each monthly cycle, and menstruation ceases. The growth of misplaced endometrial tissue usually will suppressed as well.
The goal of hormonal treatment is to simulate pregnancy or menopause, two natural conditions known to inhibit the disease. In each case, the normal endometrium is no longer stimulated to grow and regress with each monthly cycle, and menstruation ceases. The growth of misplaced endometrial tissue usually will suppressed as well.
To simulate the hormonal environment of pregnancy, birth control pills are prescribed. To be effective against endometriosis, the pills must be taken continuously without pausing for withdrawal bleeding. This state is sometimes called pseudopregnancy.
The hormone derivative danazol is the medication most frequently used to treat endometriosis. During treatment with danazol, estrogen levels are reduced to the low levels characteristic of natural menopause. This state is sometimes called pseudomenopause. Danazol is an expensive medication which is usually prescribed for six months or more. Unfortunately, large endometriotic cysts of the ovary are generally resistant to the drug.
Analogues of GnRH, the gonadotropin releasing hormone, are the newest class of hormones used for endometriosis treatment. Brand names include Lupron and Synarel. These analogues switch off production of FSH and LH from the pituitary, thus inducing a menopausal state. These analogs can be given in the form of special injections called depot preparations, which release small quantities of the drug daily, allowing administration at monthly intervals.
Medical therapy used to be prescribed in the hope that it would cause the endometriosis to shrink sufficiently so that it would no longer interfere with conception after the treatment is stopped. However, since pregnancy cannot occur during the medical therapy of endometriosis, and because the treatment has been shown not to be helpful in improving fertility, medical therapy for endometriosis is no longer advised for infertile patients.
How is surgery used for treating endometriosis ?
Surgery
Treating endometriosis with medicines has definite limitations. Medication usually controls mild or moderate pain and may eliminate small patches of the disease. But large chocolate cysts in the ovary are less likely to respond, and drugs cannot remove scar tissue. This is why surgery may be needed to improve fertility by removing adhesions, lesions, nodules or endometriomas.
As described earlier, laparoscopy can be used as a therapeutic tool. For example, fluid can be drained ; adhesions freed; and patches of endometriosis destroyed using a laser or electrical current. Even large endometriomas can be removed through the laparoscope by a skilled surgeon, so that today most cases can be successfully treated through the laparoscope. Open surgery (laparotomy) is needed only very rarely.
How is IVF used for treating endometriosis ?
IVF
Treatment cannot "cure" endometriosis - but it can control it. If an infertile woman with endometriosis fails to conceive even after surgical treatment, the next option is superovulation with intrauterine insemination, since the fallopian tubes in these patients are usually open. If this fails, then IVF ( in vitro fertilization ) can be very useful. However, the ovarian response in some of these patients can be poor, especially if they have large chocolate cysts, or have had surgery for these cysts. Fertilization rates in some patients with endometriosis can be a little lower than for other patients, perhaps because of an intrinsic oocyte abnormality.
Surgery versus IVF
I suggest that patients always test their AMH level ( a simple blood test for checking their ovarian reserve ) before allowing a doctor to do an operative laparoscopy to treat their endometriosis. This is especially true for: older women; women who have had surgery earlier; women with recurrent cysts; and women with large ovarian cysts ( because they are at risk for having poor ovarian reserve, a silent condition called oopause.) If they do have poor ovarian reserve ( as suggested by a high FSH level and a low AMH level), then surgery is not a good idea and they should move onto IVF directly.
If there is a cyst, this can always be treated by aspirating it under vaginal ultrasound guidance, so that the ovarian reserve is not further impaired.
Endometriosis is a disease affecting millions of women throughout the world. For many, the condition goes unnoticed. But for others it demands professional attention, especially when fertility is impaired. The best strategy to maximize chances of conception is to select a specialist who is familiar with the latest developments in endometriosis management.
OVARIAN CYSTS AND ENDOMETRIOSIS
Ovarian cysts are enlargements of the ovary that appear to be filled with fluid. They can be a simple fluid filled bleb or contain complex internal structures. The term cyst is used to differentiate them from solid enlargements. Simple cysts have no internal structures and are less worrisome than those with complex structures or solid components. A sonogram or ultrasound test can determine if a cyst is simple or complex.
Ovarian cysts are frequently encountered. Every menstruating woman develops an ovarian cyst each cycle. The menstrual cycle requires the coordinated functioning of the pituitary gland, ovary, uterus and the cervix. The pituitary gland in the head produces the hormones, Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH). These hormones are released into the blood stream and are the messengers that tell the ovary what to do.
The ovary responds to FSH by maturing an egg. While doing this the ovary makes and releases the hormone estrogen. The maturing egg is in a follicle cyst that grows to about one half inch in diameter. When the pituitary releases a surge of LH the follicle breaks and the egg floats out and eventually enters the tube. The remnant of the follicle cyst is called the corpus luteum and makes the hormone progesterone.
The lining of the uterus is stimulated to proliferate and grow under the influence of estrogen. Progesterone converts the lining of the uterus to become a secretory lining that is prepared to accept a pregnancy. If a pregnancy does not occur that cycle the corpus luteum stops making progesterone. When the progesterone level falls the support for the lining of the uterus is lost and it sloughs. This is the menstrual bleeding. Then the cycle starts all over again: estrogen, ovulation, progesterone and the menstrual period.
Sometimes the ovary does not ovulate and the follicle cyst persists. It will continue to enlarge and can become as big as a baseball. Eventually it will break and the woman may not even be aware that this has happened. The period may be delayed because there is no progesterone phase of the cycle to respond to. The corpus luteum can also become cystic. If these cysts are detected during an examination the woman will be told that she has a cyst. Usually this will cause considerable consternation. Now everybody is upset. Could the cyst be a cancer? Will an operation have to be done? How are these questions to be answered?
If a sonogram shows this to be a simple cyst without any internal structure.
If it is only on one side.
If it is less than 4-5 inches in diameter.
If it occurs in an ovulating woman or an early pregnant woman.
If there are no associated findings such as nodules or fluid in the pelvis.
If there are no major symptoms of pain.
Then wait.
Schedule a reexamination for 4 weeks. If it is gone or getting smaller then it was a functional cyst: either a follicle cyst or a corpus luteum cyst. Nothing more needs to be done. If it persists then a diagnosis must be arrived at surgically.
Women on birth control pills should not develop functional cysts. The function of the pill is to suppress ovulation, although some women ovulate on their pills. Premenarchal and postmenopausal women should not develop functional cysts. Women in these groups with a cyst as well as those with a complex or a solid cyst will have to be evaluated surgically. This is the only way to make sure that the cyst is or is not a cancer. A Ca-125 test is of no value. It can be elevated for a variety of reasons and a normal value is meaningless. A surgical evaluation must be done. Most of the "cysts" will be shown surgically to be things other than cancers.
In many instances, the surgical evaluation can be accomplished by laparoscopy. Laparoscopy is an outpatient procedure, but will in most cases, require a general anesthetic and a trip to the operating room.
Any ovarian or uterine enlargement in a post menopausal woman must be taken seriously. Women in this age group do not develop functional ovarian cysts. If they have fibroid tumors of the uterus these should begin to shrink at menopause. Fibroid tumors are benign tumors of the smooth muscle of the uterine wall and are common in younger women. A newly diagnosed fibroid tumor in a post menopausal woman should be an alarm signal and should be verified surgically.
ENDOMETRIOSIS
Endometriosis is a condition in which tissue similar to the lining of the uterus is located outside the uterus. Usually there are implants of this tissue in the pelvis. When the lining of the uterus bleeds during the menstrual cycle, these implants also bleed. This causes pain and scarring in the pelvis. The other pelvic structures react to this bleeding by becoming adherent to each other so that tubes, ovaries and intestine are stuck together.
If the endometrial tissue is within an ovary, that ovary will fill with blood. These are called endometriomas and are cysts in the ovary filled with old blood. This old blood has the appearance of thin chocolate or motor oil. They are also called chocolate cysts of the ovary. Endometriomas are frequently found at surgery for ovarian cysts. An elevated Ca-125 is often associated with endometriosis.
The treatment of endometriosis is usually by hormonal suppression of the menstrual cycle. This can be accomplished by using birth control pills. If the symptoms persist during the menses then the pills can be taken in a continuous fashion and not interrupted for menses. This is easily done with monophasic pills where every active pill is exactly the same. Most pills are packaged with 21 active pills followed by 7 empty or "dummy" pills.
Taking the empty pills is the same as taking no pill at all. The period only occurs when you stop taking the pill. Normally this occurs on the days when the empty pills are being taken. If the empty pills are ignored and an active pill is taken each day, then every day will be exactly the same. As long as the active pill is being taken there will be no menses. The active pills can be taken daily for as long as a year without any problem and without any bleeding.
Monophasic oral contraceptive pills each contain the same amount of an estrogen and a progestin. The net effect is that of the progestin. A continuous progesterone influence on the lining of the uterus produces thinning or atrophy of the uterine lining. This influence will also atrophy the endometrial implants.
Hormonal suppression can also be accomplished by injection of a long acting progesterone every 2 or 3 months. This drug is called Depo Provera and can be continued indefinitely. There is also a monthly injection of a GnRH type hormone. This is a Gonadotropin Releasing Hormone agonist. It basically stops all pituitary and ovarian function. It is very effective, but is useful for only 9 months at a time. There is a final solution if nothing works which is removal of the uterus and ovaries. Pregnancy also has a beneficial effect on endometriosis because it is a time of high progesterone levels.
OVARIAN CYSTS AND ENDOMETRIOSIS
Ovarian cysts are enlargements of the ovary that appear to be filled with fluid. They can be a simple fluid filled bleb or contain complex internal structures. The term cyst is used to differentiate them from solid enlargements. Simple cysts have no internal structures and are less worrisome than those with complex structures or solid components. A sonogram or ultrasound test can determine if a cyst is simple or complex.
Ovarian cysts are frequently encountered. Every menstruating woman develops an ovarian cyst each cycle. The menstrual cycle requires the coordinated functioning of the pituitary gland, ovary, uterus and the cervix. The pituitary gland in the head produces the hormones, Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH). These hormones are released into the blood stream and are the messengers that tell the ovary what to do.
The ovary responds to FSH by maturing an egg. While doing this the ovary makes and releases the hormone estrogen. The maturing egg is in a follicle cyst that grows to about one half inch in diameter. When the pituitary releases a surge of LH the follicle breaks and the egg floats out and eventually enters the tube. The remnant of the follicle cyst is called the corpus luteum and makes the hormone progesterone.
The lining of the uterus is stimulated to proliferate and grow under the influence of estrogen. Progesterone converts the lining of the uterus to become a secretory lining that is prepared to accept a pregnancy. If a pregnancy does not occur that cycle the corpus luteum stops making progesterone. When the progesterone level falls the support for the lining of the uterus is lost and it sloughs. This is the menstrual bleeding. Then the cycle starts all over again: estrogen, ovulation, progesterone and the menstrual period.
Sometimes the ovary does not ovulate and the follicle cyst persists. It will continue to enlarge and can become as big as a baseball. Eventually it will break and the woman may not even be aware that this has happened. The period may be delayed because there is no progesterone phase of the cycle to respond to. The corpus luteum can also become cystic. If these cysts are detected during an examination the woman will be told that she has a cyst. Usually this will cause considerable consternation. Now everybody is upset. Could the cyst be a cancer? Will an operation have to be done? How are these questions to be answered?
If a sonogram shows this to be a simple cyst without any internal structure.
If it is only on one side.
If it is less than 4-5 inches in diameter.
If it occurs in an ovulating woman or an early pregnant woman.
If there are no associated findings such as nodules or fluid in the pelvis.
If there are no major symptoms of pain.
Then wait.
Schedule a reexamination for 4 weeks. If it is gone or getting smaller then it was a functional cyst: either a follicle cyst or a corpus luteum cyst. Nothing more needs to be done. If it persists then a diagnosis must be arrived at surgically.
Women on birth control pills should not develop functional cysts. The function of the pill is to suppress ovulation, although some women ovulate on their pills. Premenarchal and postmenopausal women should not develop functional cysts. Women in these groups with a cyst as well as those with a complex or a solid cyst will have to be evaluated surgically. This is the only way to make sure that the cyst is or is not a cancer. A Ca-125 test is of no value. It can be elevated for a variety of reasons and a normal value is meaningless. A surgical evaluation must be done. Most of the "cysts" will be shown surgically to be things other than cancers.
CAUSES FOR AN APPARENT OVARIAN CYST Benign neoplastic ovarian cystadenomas Benign teratomas such as a dermoid Cysts of structures next to the ovary Fluid filled Fallopian tubes Infections in the tubes and or ovaries Endometriosis and endometrial ovarian cysts Fibroid tumors of the uterus that are on a stalk Abscess of the appendix Abscess of a colon diverticulum |
In many instances, the surgical evaluation can be accomplished by laparoscopy. Laparoscopy is an outpatient procedure, but will in most cases, require a general anesthetic and a trip to the operating room.
Any ovarian or uterine enlargement in a post menopausal woman must be taken seriously. Women in this age group do not develop functional ovarian cysts. If they have fibroid tumors of the uterus these should begin to shrink at menopause. Fibroid tumors are benign tumors of the smooth muscle of the uterine wall and are common in younger women. A newly diagnosed fibroid tumor in a post menopausal woman should be an alarm signal and should be verified surgically.
ENDOMETRIOSIS
Endometriosis is a condition in which tissue similar to the lining of the uterus is located outside the uterus. Usually there are implants of this tissue in the pelvis. When the lining of the uterus bleeds during the menstrual cycle, these implants also bleed. This causes pain and scarring in the pelvis. The other pelvic structures react to this bleeding by becoming adherent to each other so that tubes, ovaries and intestine are stuck together.
If the endometrial tissue is within an ovary, that ovary will fill with blood. These are called endometriomas and are cysts in the ovary filled with old blood. This old blood has the appearance of thin chocolate or motor oil. They are also called chocolate cysts of the ovary. Endometriomas are frequently found at surgery for ovarian cysts. An elevated Ca-125 is often associated with endometriosis.
The treatment of endometriosis is usually by hormonal suppression of the menstrual cycle. This can be accomplished by using birth control pills. If the symptoms persist during the menses then the pills can be taken in a continuous fashion and not interrupted for menses. This is easily done with monophasic pills where every active pill is exactly the same. Most pills are packaged with 21 active pills followed by 7 empty or "dummy" pills.
Taking the empty pills is the same as taking no pill at all. The period only occurs when you stop taking the pill. Normally this occurs on the days when the empty pills are being taken. If the empty pills are ignored and an active pill is taken each day, then every day will be exactly the same. As long as the active pill is being taken there will be no menses. The active pills can be taken daily for as long as a year without any problem and without any bleeding.
Monophasic oral contraceptive pills each contain the same amount of an estrogen and a progestin. The net effect is that of the progestin. A continuous progesterone influence on the lining of the uterus produces thinning or atrophy of the uterine lining. This influence will also atrophy the endometrial implants.
Hormonal suppression can also be accomplished by injection of a long acting progesterone every 2 or 3 months. This drug is called Depo Provera and can be continued indefinitely. There is also a monthly injection of a GnRH type hormone. This is a Gonadotropin Releasing Hormone agonist. It basically stops all pituitary and ovarian function. It is very effective, but is useful for only 9 months at a time. There is a final solution if nothing works which is removal of the uterus and ovaries. Pregnancy also has a beneficial effect on endometriosis because it is a time of high progesterone levels.
Comments
Post a Comment